Petrous Apex Disease
The petrous apex is a relatively inaccessible area that can occasionally harbor serious disease. Disease processes that usually cause symptoms are typically inflammatory or neoplastic in nature. Petrous apex lesions typically cause nonspecific symptoms such as headache, but as the lesion becomes more extensive, adjacent structures such as cranial nerves can become involved. A common early and specific sign of a petrous apex process is abducens palsy. Current imaging techniques can usually provide enough supplemental information to allow a focused plan of treatment. It is important to determine whether a petrous apex lesion can be observed or, if surgical treatment is required, whether a drainage or excision is required. There are various available surgical approaches to the petrous apex. The choice depends on the status of hearing function as well as the suspected pathology, which will dictate whether a drainage or excisional procedure is required.
- Review the anatomy of the petrous apex.
- Recognize the signs and symptoms that suggest the presence of petrous apex disease.
- Describe the normal anatomical variants of this area.
- Summarize the types of pathology that can occur in the petrous apex, the imaging required, and proper interpretation of information so that a proper differential diagnosis can be formulated.
- Formulate a plan of treatment based on clinical findings.
- Explain the various surgical approaches to the petrous apex.
Embryology
- Recognize that the embryological development of the petrous apex occurs when the temporal bone develops.
- Som PM, Curtin HD, Liu K, Mafee MF. Current Embryology of the Temporal Bone, Part 1: the Inner Ear. Neurographics. July 2016. 6(4) 250-265
Anatomy
- Identify structures that are in close relation to the petrous apex and understand how pathology in the petrous apex can affect these structures:
- Abducens nerve
- Oculomotor nerve
- Trochlear nerve
- Trigeminal nerve
- Facial nerve
- Cochleovestibular nerve
- Eustachian tube
- Cavernous sinus
- Dura of the middle and posterior cranial fossa
- Jugular foramen
- Chole RA. Petrous apicitis: surgical anatomy. Ann Otol Rhinol Laryngol 1985; 94(3):251-7
- Powell A, Kanekar S, Ghossaini S, Policare C. Petrous Apex: Anatomy and Pathologies. American Journal of Roentgenology. 2009; 192(5)
Pathogenesis
- Explain how various structural features of the petrous apex can lead to pathology in this area:
- Bone marrow versus air cells
- Drainage of petrous apex air cells
- Cartilage
- Bone
- Curtin HD, Som PM. The petrous apex.Otolaryngol Clin North Am. 1995 Jun;28(3):473-96.
- Swartz JD, Loevner LA. Imaging of the temporal bone. Pathology: Petrous Apex Lesions. 4th ed. New York: Thieme Medical Publishers, Incorporated: 2009.
Incidence
- Explain that the incidence of petrous apex lesions is low, which may lead to delay in diagnosis.
- Arriaga MA, Brackmann DE. Differential diagnosis of primary petrous apex lesions. Am J Otol 1991;12:470-74.
Patient Evaluation
- Cite that petrous apex lesions often do not cause acute and specific symptoms.
- Observe that clinical findings are related to the structures being affected.
- Identify the constellation of clinical findings usually associated with various lesions.
- Know to ask about the following symptoms when taking a history. Symptoms are related to the structures being affected and the acuteness of the process:
- diplopia, abducens palsy
- retro-orbital headache
- otorrhea
- hearing loss
- tinnitus
- otalgia
- facial numbness or pain
- dysphagia
- hoarseness
- Recognize that the otologic and cranial nerve findings are critical during a physical examination. The following findings are consistent with acute or chronic otitis media:
- cranial nerve deficits, nerves 3, 4, 5, 6, 7, 8, 9, 10, 11, 12
- meningismus
- fever
- chemosis and proptosis
- Discuss the value of an audiogram.
- Flood LM, Kemink JL. Surgery in lesions of the petrous apex. Otolaryngol Clin North Am 1984;3:565-75.
Imaging
- Explain that modern computed tomography (CT) and magnetic resonance imaging (MRI) are critical in the workup of petrous apex lesions.
- Based on CT and MRI findings, narrow the differential diagnosis so that one can determine whether the condition should be observed or whether intervention is needed.
- If intervention is needed, determine whether biopsy, drainage, or excision is required.
- Observe that CT and MRI are complementary in showing the bony and soft tissue anatomy of the area, and the combination of these studies usually allows the formulation of a narrow differential diagnosis. (see Figures 1A, B, C, Figures 2A, B, C, D, and Figures 3A, B, C, D)
- Cite that since surgical access to the petrous apex usually requires complex techniques, it is important to focus the differential diagnosis.
- Recognize that in some cases of suspected vascular lesion, a magnetic resonance angiogram (MRA) or cerebral angiogram may be required.
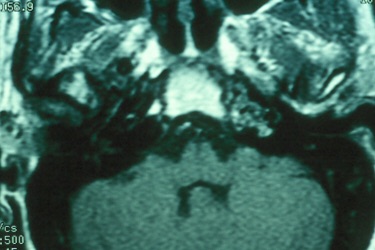

Figure 1A Figure 1B

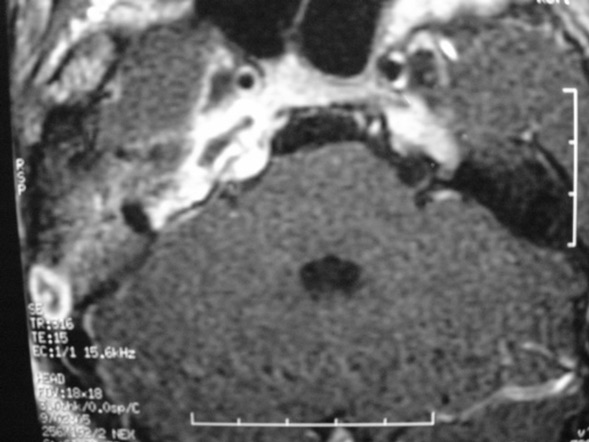
Figure 1C Figure 2A

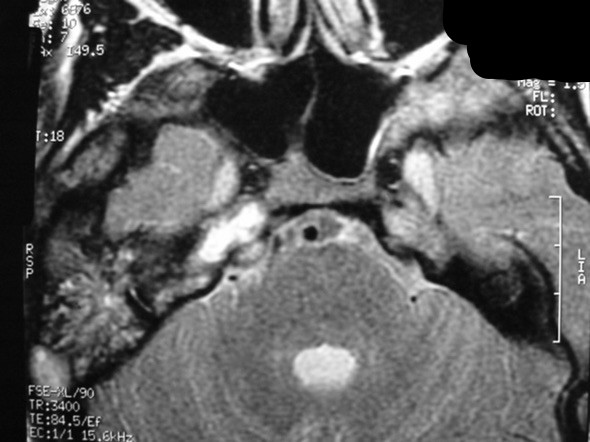
Figure 2B Figure 2C


Figure 2D Figure 3A

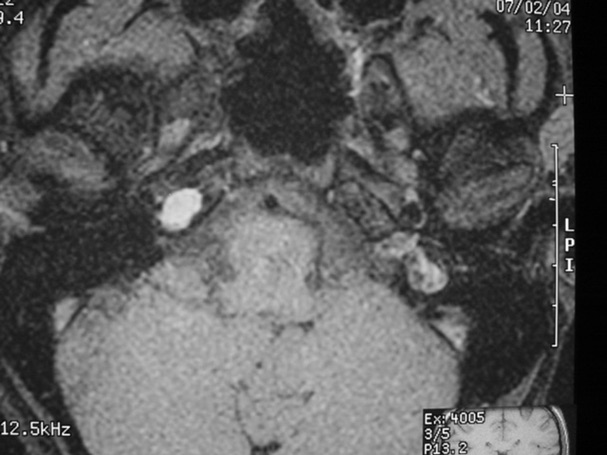
Figure 3B Figure 3C
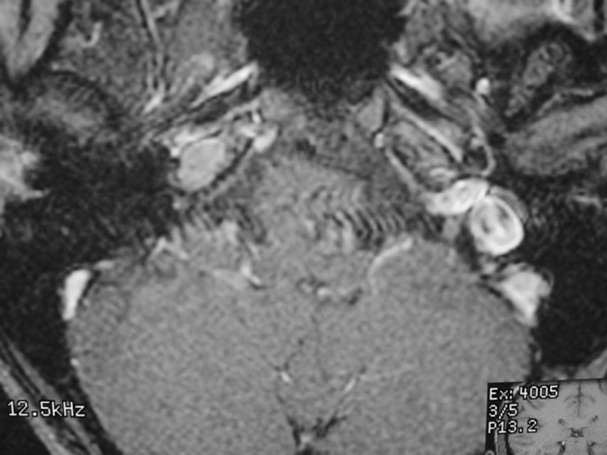
Figure 3D
- Jackler RK, Parker DA. Radiographic differential diagnosis of petrous apex lesions. Am J Otol 1992;13:561-74
- Chang CYJ. Petrous apex lesions. In: Myers EN, Alper CM, Eibling DE, editors. Decision making in ear nose and throat disorders. Philadelphia: WB Saunders Co.; 2001. p. 72-73
- Connor SEJ, Leung R, Natas S. Imaging of the petrous apex: a pictorial review. British Journal of Radiology. 2008 May;81(965):427-35
- Hentschel S, Durity F. Petrous apex granulomas: CT and MR Imaging. Canadian Journal of Neurological Sciences. 2002; 29(2): 169-170
- Schmalfuss IM. Petrous apex. Neuroimaging clinics of North America. 2009 Aug;19(3):367-91
Pathology
- Identify pathological features of lesions of the petrous apex.
- Non-neoplastic:
- effusion
- mucocele
- arachnoid cyst
- bone marrow
- cholesterol granuloma
- cholesteatoma
- petrous apicitis
- carotid aneurysm
- Neoplastic:
- chordoma
- chondrosarcoma
- osteosarcoma
- meningioma
- schwannoma
- paraganglioma
- nasopharyngeal carcinoma
- metastases
- Nager GT. Pathology of the ear and temporal bone. Baltimore: Williams & Wilkins; 1993. p. 53-62; 215-97; 178-87; 568-670; 710-814; 833-57; 903-906; 914-39
- Roseberg AE, Nielsen GP, Keel SB, et al. Chondrosarcoma of the base of skull. Am J Surg Pathol 1999 Nov;23(11):1370-8
- Powell A, Kanekar S, Ghossaini S, Policare C. Petrous apex: Anatomy and pathologies. American journal of roentgenology (1976). 2009;192(5)
Treatment
- Explain that the treatment of petrous apex lesions includes observation, medical treatment, drainage, biopsy, or excision
- Determine the appropriate treatment options for each type of lesion
- Summarize the various surgical approaches that can accomplish various treatment goals
- Identify the advantages and limitations of each surgical approach
- Chang CYJ. Petrous apex lesions. In: Myers EN, Alper CM, Eibling DE, editors. Decision making in ear nose and throat disorders. Philadelphia: WB Saunders Co.; 2001. p. 72-73
- Stevens SM, Manning A, Pensak ML, Samy RN. Long-term symptom-specific outcomes for patients with petrous apex cholesterol granulomas: Surgery versus observation. Otology & neurotology. 2017;38(2):253-259
Medical Therapies
- State that antibiotics may be appropriate in certain cases.
- Describe the evolution of medical therapy in petrous apicitis and the need of surgical intervention only in certain cases.
- Chang CYJ. Petrous apex lesions. In: Myers EN, Alper CM, Eibling DE, editors. Decision making in ear nose and throat disorders. Philadelphia: WB Saunders Co.; 2001. p. 72-73
- Gadre AK. The changing face of petrous apicitis-a 40-year experience the changing face of petrous apicitis. The Laryngoscope. 01/2018;128(1):195-201. doi: 10.1002/lary.26571
Surgical Therapies
- Summarize the surgical approaches to drainage in this area:
- infralabyrinthine
- supralabyrinthine
- subarcuate
- infracochlear
- Review the surgical approaches for excision or drainage:
- middle fossa
- translabyrinthine
- Chang CYJ. Petrous apex lesions. In: Myers EN, Alper CM, Eibling DE, editors. Decision making in ear nose and throat disorders. Philadelphia: WB Saunders Co.; 2001. p. 72-73
- Flood LM, Kemink JL. Surgery in lesions of the petrous apex. Otolaryngol Clin North Am 1984;3:565-75
- Zanation AM, Snyderman CH, Carrau RL, Gardner PA. Endoscopic endonasal surgery for petrous apex lesions. The Laryngoscope. 2009 Jan;119(1):19-25
Rehabilitation
- Explain that cranial nerve dysfunction that results from petrous apex lesions or subsequent treatment can result in significant morbidity.
- Evaluate these dysfunctions and identify treatment options:
- oculomotor dysfunction
- facial nerve dysfunction
- hearing dysfunction
- vestibular dysfunction
- voice and speech dysfunction
- dysphagia
- shoulder dysfunction
- Bennett JL, Pelak VS. Palsies of the third, fourth, and sixth cranial nerves. Ophthalmol Clin North Am 2001;14:169-85
- Freeman MS, Thomas JR, Spector JG, et al. Surgical therapy of the eyelids in patients with facial paralysis. Laryngoscope 1990;100:1086-96
- Furman JM. Dizziness. In: Myers EN, Alper CM, Eibling DE, editors. Decision making in ear nose and throat disorders. Philadelphia: WB Saunders Co.; 2001. p. 22-23
- Hirsch BE. Conductive hearing loss. In: Myers EN, Alper CM, Eibling DE, editors. Decision making in ear nose and throat disorders. Philadelphia: WB Saunders Co.; 2001. p. 2-3
- Rosen CA. Hoarseness and dysphagia. In: Myers EN, Alper CM, Eibling DE, editors. Decision making in ear nose and throat disorders. Philadelphia: WB Saunders Co.; 2001. p. 208-11
- Sabo D. Rehabilitation of hearing loss. In: Myers EN, Alper CM, Eibling DE, editors. Decision making in ear nose and throat disorders. Philadelphia: WB Saunders Co.; 2001. p. 16-17
- Zieske LA. Neck pain. In: Myers EN, Alper CM, Eibling DE, editors. Decision making in ear nose and throat disorders. Philadelphia: WB Saunders Co.; 2001. p. 282-83
Staging
- State that staging of petrous apex tumors is determined by temporal bone tumor staging.
Lionello M, Stritoni P, Facciolo MC, Staffieri A. et al. Temporal bone carcinoma. current diagnostic, therapeutic, and prognostic concepts. Journal of surgical oncology. 2014;110(4):383-392
Complications
- Indicate that petrous apex lesions can cause complications related to inflammation or compression of adjacent structures.
- Gacek RR. Diagnosis and management of primary tumors of the petrous apex. Ann Otol Rhinol Laryngol 1975;84(Suppl 18):1-20
- Grinblat G, Vashishth A, Galetti F, Caruso A. Petrous apex cholesterol granulomas: Outcomes, complications, and hearing results from surgical and wait-and-scan management. Otology & neurotology. 2017 Dec;38(10):e476-e485
Review
- What are the boundaries of the petrous apex?
- What are the normal contents of the petrous apex?
- Describe the course of all cranial nerves in relation to the petrous apex.
- What symptoms do petrous apex lesions cause?
- Describe Gradenego’s syndrome.
- When a petrous apex lesion is suspected, what imaging study should the otolaryngologist order?
- What types of lesions can occur in the petrous apex? What are the treatment options for each type of lesion? What is the most common petrous apex lesion?
- Describe the surgical approaches to the petrous apex, their indications, expected outcomes, and most common complications.
Learner must Sign In to access AAO-HNSF education activities.