Pediatric Auricular Reconstruction and Otoplasty
Pediatric Auricular Reconstruction and Otoplasty
There is a wide range of congenital auricular deformities, and mastery of their reconstruction translates well to reconstruction of traumatic or iatrogenic auricular defects as well. Recognition of which auricular structures are normal and which require reconstruction is critical to developing an appropriate plan for an individual patient. Auricular reconstruction is difficult, and patients often focus on symmetry as the primary outcome measure; it is therefore of the utmost importance to discuss realistic expectations preoperatively, especially because reconstruction of microtia is very challenging and often fraught with complications. There are multiple methods of reconstructing the auricle, ranging from non-operative techniques like ear molding and adhesive prostheses to multistage operations that require significant patient compliance with a post-operative care regimen. Each treatment plan should be tailored to the needs of the patient and take into account the advantages and disadvantages of the available techniques, the patient’s and parents’ preferences, their social situation, and their ability to comply with post-operative care instructions.
- Determine when reconstructive surgery is required to ameliorate a congenital auricular deformity.
- Identify the appropriate intervention and timing for individual patients.
- Compare and contrast different implant materials for auricular reconstruction.
Embryology
- Relate the hillocks of His to the surface anatomy of the fully developed auricle.
- Describe the progression of auricular development with respect to the outcomes of anomalies at specific points on the timeline.
- Identify the age at which the growing auricle approaches adult size.
- Weerda H. Embryology and structural anatomy of the external ear. Facial Plast Surg. 1985;2:85-91
Anatomy
- Recognize the normal surface anatomy of the fully developed auricle.
- Describe the ratio of the height to the width of a normal auricle.
- Describe the relationship of the auricle to the skull.
- Conchomastoid and auriculocephalic angles
- Location of superior and inferior poles of auricle relative to brow and nasal ala
- Posterior rotation of superior pole of auricle relative to vertical plane
- Categorize microtia according to Nagata’s system in order to identify the appropriate type of surgical reconstruction.
- Categorize other auricular deformities by name or by anatomical defect, e.g., antihelical fold deficiency (“lop ear”), conchal bowl excess, (“cup ear”) accessory antihelical crus with unfurled helical rim (“Stahl’s ear”).
- Weerda H. Embryology and structural anatomy of the external ear. Facial Plast Surg. 1985;2:85-91
- Nagata S. A new method of total reconstruction of the auricle for microtia. Plast Reconstr Surg. 1993;92(2):187-201
- Firmin F. State-of-the-art autogenous ear reconstruction in cases of microtia. Adv Otorhinolaryngol. 2010;68:25-52
- Manz RM, Wong BJ. Otoplasty: surgical correction of the prominent ear. In: Cheney ML, Hadlock TA, editors. Facial Surgery: Plastic and Reconstrctive. 2nd ed. Boca Raton: CRC Press; 2015. p.549-65.
Pathogenesis
- List prenatal risk factors that contribute to development of congenital auricular anomalies.
- Luquetti DV, Heike CL, Hing AV, et al. Microtia: epidemiology and genetics. Am J Med Genet A 158A;2011:124-39
Incidence
- Describe the incidence of microtia by laterality, sex, and race.
- Describe the incidence of prominauris.
- Luquetti DV, Heike CL, Hing AV, et al. Microtia: epidemiology and genetics. Am J Med Genet A 158A;2011:124-39
- Adamson PA, Strecker HD. Otoplasty techniques. Facial Plast Surg. 1995;11(4):284-300
Genetics
- List syndromes that may include congenital auricular deformities.
- Luquetti DV, Heike CL, Hing AV, et al. Microtia: epidemiology and genetics. Am J Med Genet A 158A;2011:124-39
Patient Evaluation
- Evaluate extent of auricular deformity and identify which structures are present and which need to be reconstructed.
- Identify other concomitant congenital anomalies that may affect the reconstructive outcome, e.g., hemifacial microsomia.
- Explain the advantages and disadvantages of different reconstructive modalities in order to determine the patient’s preferred option.
- Discuss indications for prosthesis placement.
- Discuss indications for synthetic implant placement.
- Discuss indications for reconstruction with autologous cartilage.
- Nagata S. A new method of total reconstruction of the auricle for microtia. Plast Reconstr Surg. 1993;92(2):187-201
- Thorne CH, Brecht LE, Bradley JP, et al. Auricular reconstruction: indications for autogenous and prosthetic techniques. Plast Reconstr Surg. 2001;107(5):1241-52
- Manz RM, Wong BJ. Otoplasty: surgical correction of the prominent ear. In: Cheney ML, Hadlock TA, editors. Facial Surgery: Plastic and Reconstrctive. 2nd ed. Boca Raton: CRC Press; 2015. p.549-65.
Measurement of Functional Status
- Order an audiogram for patients with microtia, particularly in cases of aural atresia.
- Jahrsdoerfer RA, Yeakley JW, Aguilar EA, et al. Grading system for the selection of patients with congenital aural atresia. Am J Otol. 1992;13(1)6-12
- Quesnel AM, Cohen MS. Otologic considerations in microtia and atresia. In: Cheney ML, Hadlock TA, editors. Facial Surgery: Plastic and Reconstrctive. 2nd ed. Boca Raton: CRC Press; 2015. p. 537-48.
Imaging
- Recognize the importance of photo-documenting the normal ear (in unilateral cases) as well as the affected ear(s) for preoperative planning.
- Consider computed tomography (CT) scanning in cases of aural atresia to determine candidacy for atresia repair.
- Manz RM, Wong BJ. Otoplasty: surgical correction of the prominent ear. In: Cheney ML, Hadlock TA, editors. Facial Surgery: Plastic and Reconstrctive. 2nd ed. Boca Raton: CRC Press; 2015. p.549-65.
- Jahrsdoerfer RA, Yeakley JW, Aguilar EA, et al. Grading system for the selection of patients with congenital aural atresia. Am J Otol. 1992;13(1)6-12
Treatment
- Determine the appropriate time to intervene in order to minimize psychological trauma to the patient but maximize chance of success.
- Consider impact of atresia repair on timing of auricular reconstruction.
- Firmin F. Ear reconstruction in cases of typical microtia. Personal experience based on 352 microtic ear corrections. Scan J Plast Reconstr Hand Surg. 1998;32(1):35-47
- Manz RM, Wong BJ. Otoplasty: surgical correction of the prominent ear. In: Cheney ML, Hadlock TA, editors. Facial Surgery: Plastic and Reconstrctive. 2nd ed. Boca Raton: CRC Press; 2015. p.549-65.
- Hadlock TA, Cheney ML, Magritz R. Microtia reconstruction. In: Cheney ML, Hadlock TA, editors. Facial Surgery: Plastic and Reconstrctive. 2nd ed. Boca Raton: CRC Press; 2015. p.521-36.
Medical Therapies
- Identify which patients are candidates for non-operative interventions, e.g., ear molding and adhesive prostheses.
- Thorne CH, Brecht LE, Bradley JP, et al. Auricular reconstruction: indications for autogenous and prosthetic techniques. Plast Reconstr Surg. 2001;107(5):1241-52
- Becon Medical, Ltd. Copyright 2010-2014. Pre Procedure Info. Video. Retrieved August, 30, 2019, from http://www.earwellsmd.com/pre-procedure-info-2/
Surgical Therapies
- Describe the process of implant placement to support an auricular prosthesis.
- Describe the stages of auricular reconstruction with a porous polyethylene implant.
- Compare and contrast the stages of auricular reconstruction with autologous costal cartilage.
- Describe the approaches reported by Tanzer and Brent.
- Describe the approaches reported by Nagata and Firmin.
- Describe common approaches to management of prominauris:
- Mustardé sutures
- Furnas sutures
- Conchal cartilage shaving
- Cartilage splitting
- “Incisionless” technique
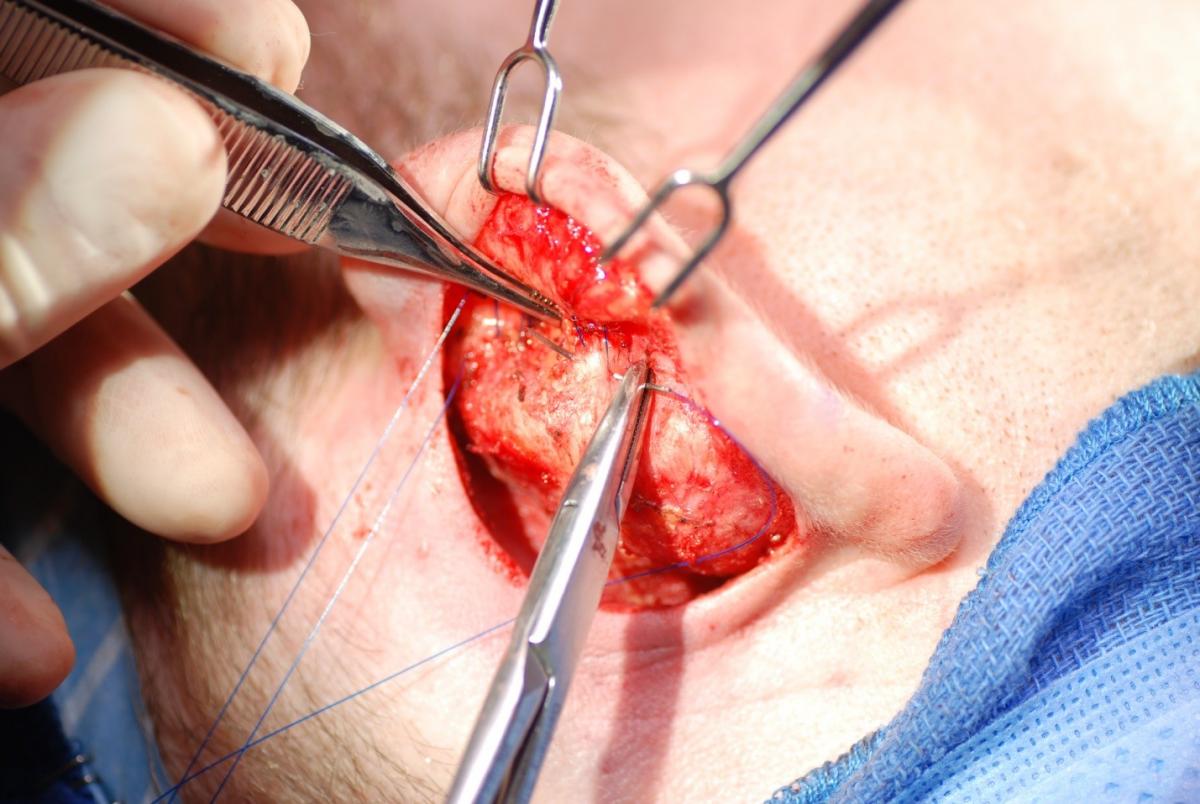
Mustardé suture placed to recreate the antihelical fold.

Furnas suture to set back the conchal cartilage.
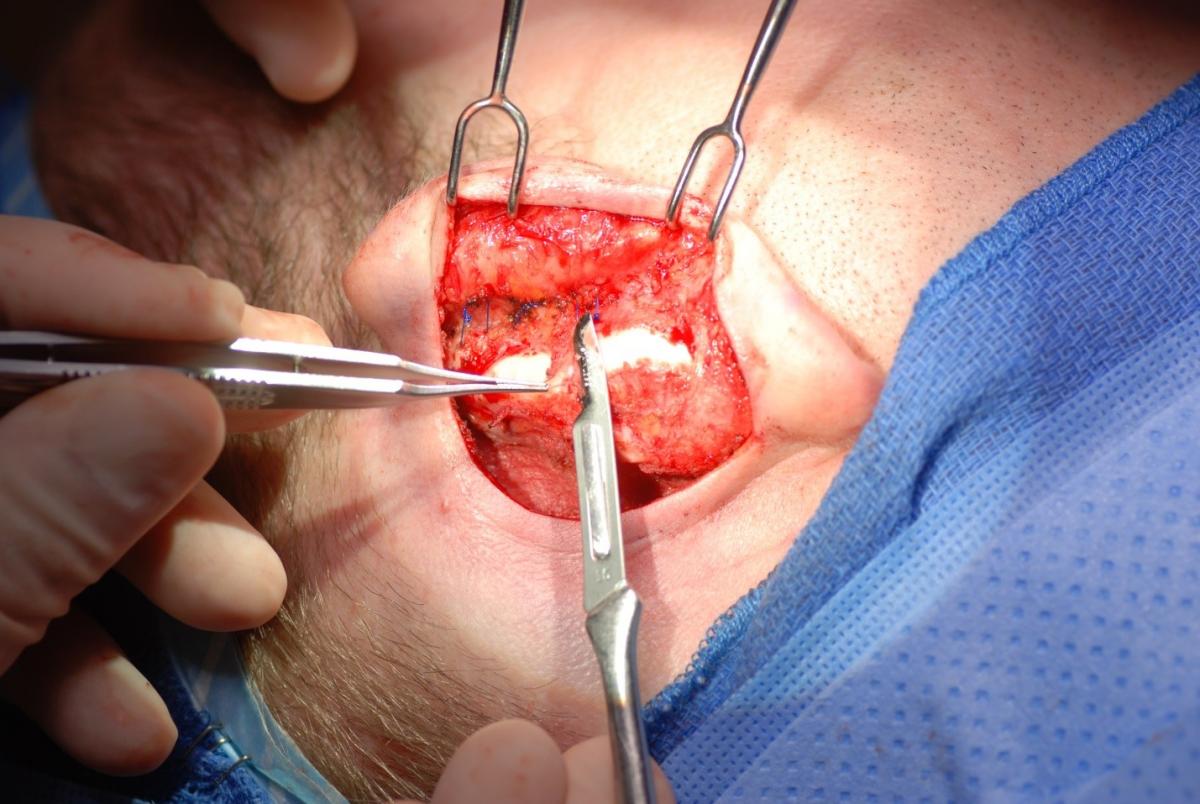
Conchal cartilage shaving to increase degree of auricular setback.
- Thorne CH, Brecht LE, Bradley JP, et al. Auricular reconstruction: indications for autogenous and prosthetic techniques. Plast Reconstr Surg. 2001;107(5):1241-52
- Berghaus A, Stelter K, Naumann A, Hempel JM. Ear reconstruction with porous polyethylene implants. Adv Otorhinolaryngol. 2010;68:53-64
- Reinisch JF, Lewin S. Ear reconstruction using a porous polyethylene framework and a temporoparietal fascia flap. Facial Plast Surg. 2009;25(3):181-9
- Tanzer RC. Total reconstruction of the external ear. Plast Reconstr Surg Transplant Bull. 1959;23(1):1-15
- Brent B. Auricular repair with autogenous rib cartilage grafts: Two decades of experience with 600 cases. Plast Reconstr Surg. 1992;90(3):355–74
- Nagata S. A new method of total reconstruction of the auricle for microtia. Plast Reconstr Surg. 1993;92(2):187-201
- Firmin F. Ear reconstruction in cases of typical microtia. Personal experience based on 352 microtic ear corrections. Scan J Plast Reconstr Hand Surg. 1998;32(1):35-47
- Mustardé JC. The correction of prominent ears using simple mattress sutures. Br J Plast Surg. 1963;16:170-8
- Furnas DW. Correction of prominent ears by conchamastoid sutures. Plast Reconstr Surg. 1968;42(3):189-193
- Nachlas NE, Duncan D, Trail M. Otoplasty. Arch Otolaryngol. 1970;91(1):44-9
- Mehta S, Gantous A. Incisionless otoplasty: a reliable and replicable technique for the correction of prominauris. JAMA Facial Plast Surg. 2014;16(6):414-8
Rehabilitation
- Describe the role of adjunctive procedures after completion of the microtia reconstruction, e.g., LASER hair removal.
- Takase M, Hashimoto I, Nakanishi H, et al. Reconstruction of microtia with laser hair removal before transplantation of costal cartilage. J Plast Reconstr Aesthet Surg. 2008;61 Suppl 1:S86-91
- Firmin F. State-of-the-art autogenous ear reconstruction in cases of microtia. Adv Otorhinolaryngol. 2010;68:25-52
Staging
- Describe the Marx classification of microtia.
- Correlate the Nagata classification of microtia to the appropriate surgical reconstructive plan.
- Marx H. Die Missbildungen des ohres. In: Denker AK, editor. Handbuch der Spez Path Anatomie Histologie. Berlin: Springer; 1926. p. 131.
- Nagata S. A new method of total reconstruction of the auricle for microtia. Plast Reconstr Surg. 1993;92(2):187-201
Case Studies
- An 11-year-old Hispanic male presents for treatment of congenital right-sided auricular deformity. He is otherwise healthy and has never had surgery. Physical examination reveals grade III microtia of the right ear with external auditory canal atresia and a normal left auricle. The tympanic membrane appears normal; there is no hemifacial microsomia or facial palsy. There is a strong superficial temporal artery pulse and the chest wall appears normal. The patient’s parents express a preference for the use of autologous cartilage in the reconstruction. How do you proceed to manage this patient’s microtia?
- Preoperative evaluation should include audiometry and photography of both auricles as well as a CT scan.
- The Brent method of costochondral auricular reconstruction is a four stage procedure: harvest of the seventh-eighth rib synchondrosis and the ninth to fashion the helical rim, with fabrication and placement of the cartilage construct at the site of the microtic auricle; transposition of the lobule with a z-plasty and removal of remnant cartilage; elevation of the neo-auricle and application of a split thickness skin graft to the posterior surface; and then reconstruction of the tragus with a composite graft from the contralateral conchal bowl.
- The Nagata method is a two stage repair: the sixth through ninth costal cartilages are harvested and used to create a construct that includes a tragus, which is then placed at the site of the microtic auricle at the same time that the lobule transposition is performed; the auricle is later elevated and a temporoparietal fascia flap is transferred to the postauricular area and covered with a split thickness skin graft.
- Two weeks after completion of the final stage of the reconstruction, the patient is struck in the neo-auricle with a football. Over the next several days, the cartilage at the superior helix becomes exposed and the wound begins to drain. What options are available to treat the new defect?
- Culture of the wound may reveal Pseudomonas aeruginosa infection, which warrants treatment with a fluoroquinolone or third generation cephalosporin. The cartilage should also be covered with vascularized tissue to prevent resorption, often with more temporoparietal fascia or occipitoparietal fascia.
- After resolution of the wound complication and sufficient time for recovery from the last stage of the reconstruction, repair of the external auditory canal atresia can be undertaken.
- An eight day old infant presents for treatment of a congenital left-sided auricular deformity. She is otherwise healthy. Physical examination reveals a Stahl’s ear without external auditory canal atresia and a normal right auricle. The tympanic membrane appears normal. Are there any non-invasive options to correct this auricular deformity?
- Stahl’s ear is a deformity in which there is a third, vertically-oriented crus of the antihelix that unfurls the helical rim where the two structures meet. The remainder of the auricle is normal; all other surface anatomy is unaffected.
- In a patient with otherwise normal auricular anatomy, molding of the cartilage may be considered if performed early enough. The usual threshold for attempting auricular molding is before three weeks of life.
- The mold is applied with an adhesive and the auricle checked to ensure the skin is not blanching due to pressure from the molding apparatus.
- The patient is seen every two weeks for reapplication of the apparatus; the course of treatment is typically six weeks long.
- A 10-year-old female presents for treatment of bilateral congenital auricular deformities; she and her parents are concerned that she will be ridiculed because of the size of her ears when she starts middle school next year. She is otherwise healthy and has never had surgery. Physical examination reveals bilateral antihelical deficiency and conchal bowl excess. Her auricular measurements are as follows: right side – superior 30 mm, middle 32 mm, inferior 33 mm; left side – superior 25 mm, middle 28 mm, inferior 30 mm.
- Preoperative evaluation should include photography.
- Schedule the procedure for a time when the patient will be able to comply with the post-operative care regimen of headband wear without attracting attention from her peers, usually over the summer.
- Counsel the patient and parents that the auricles are asymmetric preoperatively and that the goal will be to restore symmetry to below the threshold for detection by a casual observer, roughly 3 mm of difference between sides.
- The otoplasty should include both Mustardé and Furnas sutures, placed more aggressively on the right side, and possibly conchal cartilage shaving. Place the Mustardé sutures before the Furnas sutures, because access to the posterior auricle becomes more challenging after the auricular setback.
- The goal should be for the post-operative measurements to be as follows: superior 10-15 mm, middle 15-20 mm, inferior 15-20 mm, with a 3 mm or less difference between the left and right auricles. Slight overcorrection will compensate for postoperative stretching of the sutures and widening of the auriculocephalic angle.
- On post-operative day one, the patient complains of pain and swelling of the left auricle. Physical examination reveals significant ecchymosis, edema, tenderness, and prominauris of the left auricle with dark blood draining from the incision.
- Drainage of the hematoma and replacement of a pressure dressing should resolve the issue. Placing small drains into the postauricular incisions at the time of surgery may help prevent hematoma formation.
- Three months later, the patient complains of a painful nodule on the posterior aspect of the right auricle. Physical examination reveals a suture granuloma.
- Removal of the suture resolves the issue and the auricle retains its shape due to scar tissue formation. If the offending suture must be removed in the early post-operative period, the auricle may revert partially to its preoperative shape and require a future revision.
- Hadlock TA, Cheney ML, Magritz R. Microtia reconstruction. In: Cheney ML, Hadlock TA, editors. Facial Surgery: Plastic and Reconstrctive. 2nd ed. Boca Raton: CRC Press; 2015. p.521-36.
- Becon Medical, Ltd. Copyright 2010-2014. Ear Well MD Home. Retrieved August, 30, 2019, from http://www.earwellsmd.com/?loggedin
- Manz RM, Wong BJ. Otoplasty: surgical correction of the prominent ear. In: Cheney ML, Hadlock TA, editors. Facial Surgery: Plastic and Reconstrctive. 2nd ed. Boca Raton: CRC Press; 2015. p.549-65.
Complications
- Discuss the etiology of wound breakdown and implant exposure and cartilage resorption.
- Identify most common bacteria associated with wound infection.
- Discuss options to provide additional soft tissue coverage of the reconstruction.
- Prepare to counsel patients about possible sources of post-operative dissatisfaction and what additional interventions may be required.
- Recognize risk factors for developing post-operative complications.
- Describe realistic outcomes in terms of ultimate appearance of an operated auricle and symmetry with respect to the contralateral side.
- Describe common surgical errors in otoplasty.
- Telephone ear, external auditory meatus stenosis
- Describe deformities that may arise due to post-operative hematoma, infection, or suture extrusion.
- Firmin F. State-of-the-art autogenous ear reconstruction in cases of microtia. Adv Otorhinolaryngol. 2010;68:25-52
- Hadlock TA, Cheney ML, Magritz R. Microtia reconstruction. In: Cheney ML, Hadlock TA, editors. Facial Surgery: Plastic and Reconstrctive. 2nd ed. Boca Raton: CRC Press; 2015. p.521-36.
- Manz RM, Wong BJ. Otoplasty: surgical correction of the prominent ear. In: Cheney ML, Hadlock TA, editors. Facial Surgery: Plastic and Reconstrctive. 2nd ed. Boca Raton: CRC Press; 2015. p.549-65.
Review
- What are the advantages and disadvantages of different methods of reconstructing an auricle?
- What is the optimal age to begin a reconstruction with a prosthesis/synthetic implant? A costal cartilage reconstruction?
- What are the stages of costal cartilage reconstruction?
- What is the maximum age to attempt non-operative ear molding?
- What are the options for salvaging a reconstruction in the event of wound breakdown and implant exposure/cartilage resorption?
- Thorne CH, Brecht LE, Bradley JP, et al. Auricular reconstruction: indications for autogenous and prosthetic techniques. Plast Reconstr Surg. 2001;107(5):1241-52
- Hadlock TA, Cheney ML, Magritz R. Microtia reconstruction. In: Cheney ML, Hadlock TA, editors. Facial Surgery: Plastic and Reconstrctive. 2nd ed. Boca Raton: CRC Press; 2015. p.521-36.
- Manz RM, Wong BJ. Otoplasty: surgical correction of the prominent ear. In: Cheney ML, Hadlock TA, editors. Facial Surgery: Plastic and Reconstrctive. 2nd ed. Boca Raton: CRC Press; 2015. p.549-65.
- Brent B. Auricular repair with autogenous rib cartilage grafts: Two decades of experience with 600 cases. Plast Reconstr Surg. 1992;90(3):355–74
- Nagata S. A new method of total reconstruction of the auricle for microtia. Plast Reconstr Surg. 1993;92(2):187-201
- Becon Medical, Ltd. Copyright 2010-2014. Ear Well MD Home. Retrieved August, 30, 2019, from http://www.earwellsmd.com/?loggedin