Acquired Laryngotracheal Diseases
Acquired laryngotracheal diseases in children are becoming increasingly common with the salvage of younger-gestation neonates of low birth weight. Though challenging, reconstructive techniques are available to correct even the most significant degrees of subglottic stenosis if appropriate diagnoses are made and proper patient selection is exercised. Infectious and inflammatory diseases are also treatable with prompt recognition and appropriate airway stabilization in conjunction with medical therapy. A more challenging situation exists for managing diseases, such as recurrent respiratory papillomatosis, where the virus is latent in the larynx and surgery is not curative.
After completing this module, the physician will be able to:
- Differentiate between infectious, inflammatory, neurogenic, and traumatic causes of airway obstruction from acquired laryngotracheal diseases.
- Review the relative incidence of infectious and inflammatory causes of airway obstruction by age.
- Explain the pathophysiology and underlying anatomic factors that contribute to the development of subglottic stenosis in the neonatal airway.
- Describe the different options and approaches for medical and surgical management of children with acquired subglottic stenosis and the benefits in choosing one particular treatment plan over another.
- Recognize the signs and symptoms, etiology, and management strategies in diagnosing and treating recurrent respiratory papillomatous disease.
Anatomy
Anatomy Understand how the pediatric and adult larynx differ in size and location and the implications of these differences on:
- the development of subglottic stenosis.
- risk of traumatic injury to the laryngotracheal complex.
- the effect of circumferential mucosal edema in narrowing the subglottic lumen.
- the cricoid cartilage, the only point in the airway that is completely surrounded by cartilage.
- Rutter MJ, Cotton RT. Laryngeal stenosis. In: Bailey, BJ. Head and neck surgery – otolaryngology. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2006. p. 881-93.
- Willging JP, Cotton RT. Subglottic stenosis in the pediatric patient. In: Myer CM, Cotton RT, Shott SR, eds. The pediatric airway: an interdisciplinary approach. Philadelphia: JB Lippincott; 1995. p. 111-32.
Pathogenesis
Understand how laryngeal and subglottic/tracheal stenosis may occur as a consequence of:
- past endotracheal intubation
- related to time intubated, type of tube, movement of the tube, presence of reflux, and superimposed bacterial or viral infections.
- ischemic necrosis from pressure of tube against a narrowed subglottic space and cricoid cartilage.
2.prior surgical interventions.
- related to cautery, laser, radiation, or thermal damage or other iatrogenic trauma.
- related to failed attempts at laryngotracheal reconstruction.
- related to high tracheotomy or cricothyrotomy.
3. infectious or inflammatory disorders.
- as a result of end-stage processes of untreated disease.
- as a consequence of prior disease treatment (i.e., development of anterior commissure webbing from overly zealous removal of papillomas).
- Cotton RT. Management and prevention of subglottic stenosis in infants and children. In: Bluestone CD, Stool SE, editors. Pediatric otolaryngology. 4th ed. 2002, WB Saunders. Phildadelphia, PA. p. 1194-204.
Incidence
Understand that the frequency with which different infectious and inflammatory conditions of the larynx occurs are dependent on the age of the child, his/her immune status, other underlying medical conditions, and unknown risk factors.
- Infectious causes of laryngotracheal diseases.
- Croup.
- Viral laryngotracheobronchitis: > 95% of cases, typically infants from 6 months to 2 years, most commonly in winter and early spring, classic “steeple sign” on anterior/posterior neck plain films; if recurrent or persistent consider endoscopy to rule out an underlying anatomic abnormality by visualization of the airway.

- Spasmodic: no prodromal illness but typically occurs in the middle of the night, older children, may be related to gastroesophageal reflux disease (GERD), stress, allergy, or temperature changes.
- Viral laryngotracheobronchitis: > 95% of cases, typically infants from 6 months to 2 years, most commonly in winter and early spring, classic “steeple sign” on anterior/posterior neck plain films; if recurrent or persistent consider endoscopy to rule out an underlying anatomic abnormality by visualization of the airway.
- Epiglottitis.
- Young children between 2 and 7 years but now becoming very rare because of near-universal vaccination against Haemophilus influenzae type b (HiB).

- Rarely seen but more frequent now in older children and adults because of non-typeable H. influenzae and other organisms but less severe of a disease process.
- Young children between 2 and 7 years but now becoming very rare because of near-universal vaccination against Haemophilus influenzae type b (HiB).
- Bacterial tracheitis.
- Associated with a recent upper respiratory infection or as a complication of another infection: Staphylococcus aureus,(methicillin-resistance and multi-drug resistance more common now), Moraxella catarrhalis GABHS, H. influenzae are the most common organisms.
- Bronchoscopy may be therapeutic as well as diagnostic.
- Recurrent respiratory papillomatosis.

- 75% diagnosed by 5 years of age with most common presentation in 2- to 5-year-olds. Classic triad of first born to young, sexually active mother delivered vaginally. Caused by HPV 6 and 11. Recurrences due to latent infection in surrounding tissues with predilection for areas of stratified squamous epithelium and iatrogenic areas of squamous metaplasia.
- Juvenile form tends to be more aggressive than the adult form and leads to a greater need for frequent surgery, adjuvant medical therapy, and tracheotomy.
- Bronchiolitis: acute respiratory illness affecting young infants causing inflammation and obstruction in the small bronchioles. Most commonly caused by respiratory syncytial virus. A major cause of morbidity and mortality in infants with underlying and congenital cardiopulmonary problems.
- Other viral, bacterial, fungal, and mycobacterial infections.
- Diphtheria, tuberculosis (typical and atypical), herpes, varicella, mucocutaneous candidiasis, histoplasmosis, pertussis.
- Diphtheria, tuberculosis (typical and atypical), herpes, varicella, mucocutaneous candidiasis, histoplasmosis, pertussis.
- Croup.
- Inflammatory causes of laryngotracheal diseases.
- Juvenile rheumatoid arthritis: autoimmune disease affecting children of all ages producing airway compromise due to involvement of the cricoarytenoid joint causing decreased abduction of the vocal folds.
- Dermatomyositis: inflammatory disease of striated muscle and skin with obliterative vasculitis involving small vessels.
- Allergic bronchopulmonary aspergillosis: usually occurs in atopic and asthmatic children.
- Pemphigus vulgaris: occasionally seen in children, affects cutaneous and mucosal surfaces.
- Bullous pemphigoid: an autoimmune disorder seen more frequently in the elderly but can occur in infants and young children. Mucosal involvement with blistering may cause upper airway obstruction.
- Stevens-Johnson syndrome: a form of erythema multiforme characterized by extensive mucosal erosions. More common in children than in adults and typically affects teenagers. Associated with immune response to a precipitating factor such as antibiotics.

- Anaphylaxis: a type 1 allergic reaction involving immunoglobulin E associated with allergic angioedema causing airway obstruction. Requires immediate treatment including securing the airway, administration of epinephrine, antihistamines, fluid resuscitation, H2 blockers, and corticosteroids. Prevention is critical in preventing subsequent episodes.
- Hereditary angioedema: a defect of the complement system involving a defect in C1 inhibitor, can occur in children as young as 2 years, related to precipitating factors such as airway trauma. Typically presents with multiple episodes of angioedema necessitating treatment.
- Wegener’s granulomatosis: a necrotizing vasculitis affecting the respiratory mucosa, more typically in the nose but also involving the larynx or subglottis.
- Polychondritis: autoimmune disorder typically involving the cartilage of the nose and ear in teenagers and young adults but also can involve the cricoid cartilage producing subglottic stenosis or vocal cord immobility
3. Acquired neurogenic
- Traumatic: due to birth injury or as a consequence of surgery for cardiovascular or esophageal anomalies.
- Infectious: postnatal infections such as polio, rabies, Guillain-Barré, tetanus, botulism, syphilis, HIV, myasthenia gravis and polyneuritis may cause airway obstruction from their effects on cranial nerve X (vagus nerve)
- Supranuclear: multiple sclerosis and kernicterus can also cause neurogenic deficits in children.
4.Trauma.
- Blunt and penetrating trauma are relatively rare because of the anatomy of the infant and pediatric airway. Clothesline injury (with potential for laryngotracheal separation), attempted suicide by hanging, and blunt trauma from striking anterior neck on objects such as coffee tables, sporting equipment (hockey puck, stick, ball) are most common presentations.
- Thermal injury: may occur at any age from steam, fire, or iatrogenic from laser airway fire.
- Caustic ingestion: may occur from either acidic or alkaline ingestions.
- Reflux: seems disproportionately present in children with subglottic stenosis, causes edema, erythema, mucosal posterior pharyngeal cobblestoning and “active” larynx appearance.
- Iatrogenic: can occur because of wrong size endotracheal tube or traumatic intubation with dislocation of arytenoids.
- Radiation effects: may occur in the context of treatment for laryngeal malignancies.
- Foreign body in the airway: Most common entities are vegetable products such as peanuts and seeds. Other foods include popcorn, hot dogs, grapes. Most lethal are conforming foreign bodies such as balloons. Foreign bodies such as batteries in the airway can cause obstruction and caustic injury from the acidic nature of the battery.
5. Postintubation stenosis.
- Associated with advent of neonatal and pediatric intensive care units and salvage of low-birthweight infants with bronchopulmonary dysplasia and children with congenital anomalies requiring prolonged ventilatory support or airway stenting.
- Related to tube size, movement, length of intubation, and associated inflammatory factors as well as intrinsic healing re-epithelialization in the cricoid region.
6. Postoperative stenosis.
- Related to high tracheotomies, cricothyrotomy. or improper tracheotomy care. Although cricothyrotomy may be a life-saving procedure in the emergency room or out in the field, it has a high complication rate in children and should be converted to a tracheotomy as soon as patient is stable and it is possible to limit stenosis risk.
- Related to failed attempts at laryngotracheal reconstruction or any airway surgery occurring in the presence of an active larynx (uncontrolled reflux or infection).
- Cressman WR, Myer CM III. Diagnosis and management of croup and epiglottitis. Pediatr Clin North Am 1994;41:265-76.
- Cunningham M. The old and new of acute laryngotracheal infections. Clin Pediatr 1992;31: 56-66.
- Derkay CS. Recurrent respiratory papillomatosis. Laryngoscope 2001;111:57-69.
- Derkay CS. Task force on recurrent respiratory papillomas. Arch Otolaryngol Head Neck Surg 1995;121:1386-91.
- Lepow ML, Hetherington S. Infections of the lower respiratory tract. In: Bluestone CD, Stool SE, editors. Pediatric otolaryngology. 4th ed, WB Saunders, Philadelphia, 2002. p. 1152-60.
- Sie KCY. Infectious and inflammatory disorders of the larynx and trachea. In: Wetmore R, Muntz H, McGill T, editors. Pediatric otolaryngology. New York: Thieme; 2000. p. 811-25.
Patient Evaluation
- Understand that the history is often the key feature of evaluation supplemented by a careful physical examination and an endoscopic examination of the airway to confirm the findings.
- Know that laboratory testing may be useful in the setting of infectious and inflammatory diseases.
- Know that the history should be directed at determining the degree of airway obstruction, duration of symptoms, associated illnesses, and risk factors.
- Symptoms of importance to elicit are noisy breathing, retractions, color changes, air hunger, use of accessory respiratory muscles, feeding difficulties, failure to thrive, voice changes, disturbed sleep, possibility of foreign body aspiration, and past history of surgeries and/or intubations.
- Understand that the physical examination should be directed at determining the severity of the illness to determine the urgency of action. Includes noting vital signs (including pulse oximetry); observing the child breathing pattern and listening for stridor, stertor, and noisy breathing; observing the patient’s neck, chest wall, and degree of accessory respiratory muscle use and auscultation of the lungs.
- Know that flexible fiberoptic laryngoscopy may be undertaken to assess the larynx, hypopharynx, and nasopharynx but only if the patient is stable and appropriate equipment and personnel are available for intervention if the airway becomes more compromised.
- Understand that laboratory studies may include cultures or biopsies of the involved areas to confirm a diagnosis.
- Blood tests specific to certain diagnoses are sometimes indicated.
- Albert D, Leighton S. Stridor and airway management. In: Cummings CW, Haughey BH , Harker LA, et al., editors. Pediatric otolaryngology head & neck surgery. 4th ed. St. Louis: Mosby; 2004. p. 285-302.check pages
- Daniel SJ. The upper airway: congenital malformations. Pediatr Respir Rev 2006;7;Suppl 1:S260-3.
- Zalzal GH. Stridor and airway compromise. Pediatr Clin North Am 1989;36:1389-1401.
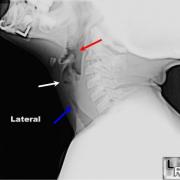
Imaging
- Know that imaging studies may play a role in identifying the site of lesion as well as ruling out extrinsic and intrinsic lesions compressing the airway.
- Understand the role that plain radiographs of the neck and/or chest, fluoroscopy with or without barium, and occasionally the use of computed tomography and/or magnetic resonance imaging plays to assess for extrinsic masses impacting the airway.
- Albert D, Leighton S. Stridor and airway management. In: Cummings CW, Haughey BH , Harker LA, et al., editors. Pediatric otolaryngology head & neck surgery. 4th ed. St. Louis: Mosby; 2004. p. 285-302.check pages
- Pransky SM. Evaluation of the compromised neonatal airway. Pediatr Clin North Am 1989;36:1571-83.
Pathology
- Histologic examination of tissue may be necessary for confirmation of diagnosis in papilloma disease, other benign and malignant neoplasms, and in some inflammatory lesions.
- Albert D, Leighton S. Stridor and airway management. In: Cummings CW, Haughey BH , Harker LA, et al., editors. Pediatric otolaryngology head & neck surgery. 4th ed. St. Louis: Mosby; 2004. p. 285-302.
Treatment
- Understand that the treatment of acquired laryngotracheal diseases is dependent on the etiology, location, and the degree of airway obstruction.
- In some cases, observation, medical management, and airway monitoring alone are sufficient because the natural history is benign, while other situations may require interventions including tracheotomy and subsequent laryngotracheal reconstruction.
- Stroud RH, Friedman NR. An update on inflammatory disorders of the pediatric airway: epiglottitis, croup and tracheitis. Am J Otolaryngol 2001; 22; 268-75.
- Sie KCY. Infectious and inflammatory disorders of the larynx and trachea. In: Wetmore R, Muntz H, McGill T, editors. Pediatric otolaryngology. New York: Thieme; 2000. p. 811-25.
Medical Therapies
- Understand the role of prevention through the use of vaccines against HiB and HPV.
- Recognize the potential benefits of ancillary medical management of coinciding disorders, such as GERD and asthma, in the treatment of children with subglottic stenosis.
- Appreciate the benefits of nonmedical therapies such as humidification and fluid resuscitation in the treatment of these children.
- Understand the role of antibiotics and antiviral agents in the specific treatment of infectious disorders affecting the larynx and trachea.
- Recognize the choices of adjuvant therapies for treatment of recurrent respiratory papillomatosis and the limited number of evidence-based, well-controlled studies demonstrating their efficacy, including alfa-interferon, cidofovir, ribavirin, photodynamic therapy, and indole-3-carbinol.
- Stroud RH, Friedman NR. An update on inflammatory disorders of the pediatric airway: epiglottitis, croup and tracheitis. Am J Otolaryngol 2001; 22; 268-75.
- Sie KCY. Infectious and inflammatory disorders of the larynx and trachea. In: Wetmore R, Muntz H, McGill T, editors. Pediatric otolaryngology. New York: Thieme; 2000. p. 811-25.
- Derkay CS, Darrow DH. Recurrent respiratory papillomatosis. Ann Otol Laryngol Rhinol 2006, 115, 1-11.
- Freed GL, Derkay CS. Prevention of recurrent respiratory papillomatosis: role of HPV vaccination. Int J Pediatr Otorhinolaryngol 2006; 70; 1799-803.
- Shikowitz MJ, Abramson AL, Steinberg BM et al. Clinical trial of photodynamic therapy with meso-tetra (hydroxyphenyl) chlorin for respiratory papillomatosis. Arch Otolaryngol Head Neck Surg 2005; 131; 99-105.
Pharmacology
- Recognize the appropriate antibiotics to utilize to cover the most common organisms that cause epiglottitis, bacterial tracheitis, and other bacterial cause of airway obstruction.
- Understand the potential role of corticosteroids and mitomycin C in the treatment of subglottic stenosis and airway edema.
- Understand the role of bevacizumab in the treatment of aggressive papillomatous disease.
- Stroud RH, Friedman NR. An update on inflammatory disorders of the pediatric airway: epiglottitis, croup and tracheitis. Am J Otolaryngol 2001; 22; 268-75.
- Hartnick CJ, Hartley BE, Lacy PD. Liu J et al. Topical mitomycin application after laryngotracheal reconstruction: a randomized, double-blind, placebo-controlled trial. Arch Otolaryngol Head Neck Surg, 2001; 127; 1260-4.
- Derkay CS, Darrow DH. Recurrent respiratory papillomatosis. Ann Otol Rhinol Laryngol 2006; 115; 1-11.
- Shikowitz MJ, Abramson AL, Freeman K, et al. Efficacy of DHE photodynamic therapy for respiratory papillomatosis; immediate and long-term results. Laryngoscope 1998;108:962-67.
- Shikowitz MJ, Abramson AL, Steinberg BM et al. Clinical trial of photodynamic therapy with meso-tetra (hydroxyphenyl) chlorin for respiratory papillomatosis. Arch Otolaryngol Head Neck Surg 2005; 131; 99-105.
- Zur KB, Fox E. Bevacizumab chemotherapy for management of pulmonary and laryngotracheal papillomatosis in a child. Laryngoscope. 2017 Jul;127(7):1538-1542. doi: 10.1002/lary.26450. Epub 2016 Dec 20.
Surgical Therapies
- For subglottic stenosis, recognize that tracheotomy can often be the most conservative means of treatment by securing the airway and removing the inflammatory effect of the endotracheal tube on the creation of subglottic and glottic mucosal injury.
- Understand the role of anterior cricoid split in the neonate who fails to extubate.
- Understand the potential role of balloon dilation for less severe forms of subglottic stenosis and for post-operative management after laryngotracheal reconstruction.
- Understand the indications for and technical differences involved in the use of each of the following techniques of laryngotracheal reconstruction:
- anterior graft.
- anterior graft with posterior split.
- posterior graft.
- anterior and posterior graft.
- cricotracheal resection.
- Slide tracheoplasty
- Resection and end-to-end re-anastomosis for tracheal stenosis
- Recognize the indications, benefits, and differences between single-stage reconstruction and two-stage reconstruction.
- Recognize the controversies surrounding choice of stents and length of stenting.
- Recognize the role of reflux control, management of lower airway disease. and treatment of concomitant bacterial infection in maximizing the success of reconstruction.
- For recurrent respiratory papillomatosis, recognize the limitations of surgical debulking in the treatment of this disease caused by a latent viral infection.
- Understand the choices of surgical methods of debulking including:
- “cold steel” (microlaryngoscopy techniques)
- carbon dioxide laser.
- KTP laser.
- pulse dye laser.
- microdebriders.
- Cotton RT. The problem of pediatric laryngotracheal stenosis; a clinical and experimental study on the efficacy of autogenous cartilaginous grafts placed between the vertically divided lamina of the cricoid cartilage. Laryngoscope 1991;(Suppl 56):1-49.
- Derkay CS, Darrow DH. Recurrent respiratory papillomatosis. Ann Otol Rhinol Laryngol 2006; 115;1-11.
- Derkay CS. Task force on recurrent respiratory papillomas. Arch Otolaryngol Head Neck Surg 1995;121:1386-91.
- Myer CM III, O’Connor DM, Cotton RT. Proposed grading system for subglottic stenosis based on endotracheal tube sizes. Ann Otol Rhinol Laryngol 1994;103:319-24.
- Seid AB, Pransky SM, Kearns DB. One stage laryngotracheoplasty. Arch Otolaryngol Head Neck Surg 1991;117:408-15.
- Zalzal GH. Stenting for pediatric laryngotracheal stenosis. Ann Otol Rhinol Laryngol 1992;101:651-55.
- White DR, Cotton RT, Bean JA, Rutter MJ. Pediatric cricotracheal resection: surgical outcomes and risk factor analysis. Arch Otolaryngol Head Neck Surg; 2005;131;896-9.
- Cotton RT. Management of subglottic stenosis. Otolaryngol Clin North Am 2000; 33;111-30.
- Rutter MJ, Vijayasekaran S, Salamone FN et al. Deficient tracheal rings. Intl J Pediatr Otorhinolaryngol 2006; 70;1981-4.
Staging
- Recognize the importance of nomenclature in presenting results of therapy and discussing patient management between healthcare providers.
- Know that staging systems have been developed and widely adopted to describe the degree of narrowing in the subglottis/glottis in the case of stenosis and throughout the aerodigestive tree for papilloma.
- For subglottic stenosis, recognize the value and significance of the Cotton/Myer grading scale to describe subglottic stenosis.
- For papilloma, recognize the value and significance of the Coltrera/Derkay and Kashima grading scales.
- Derkay CS, Malis D, Zalzal G, et al. A staging system for assessing severity of disease and response to therapy in recurrent respiratory papillomatosis. Laryngoscope 1998; 108:935-37.
- Kashima H, Leventhal B, Mounts P. Papilloma Study Group. Scoring system to assess severity and course in recurrent respiratory papillomatosis. In: Howley PM, Broker TR, editors. Papillomavirus: molecular and clinical aspects. New York: Alan R Liss; 1985. p. 125-35.
- Myer CM III, O’Connor DM, Cotton RT. Proposed grading system for subglottic stenosis based on endotracheal tube sizes. Ann Otol Rhinol Laryngol 1994;103:319-24.
Case Studies
- Infectious disorder: An 18-month-old boy presents to your office after experiencing his 6th episode of croup that required a visit to the emergency department and treatment with racemic epinephrine and corticosteroids. He is completely asymptomatic between episodes. Each episode has begun with a viral prodrome. He has never been intubated, was full-term, and is otherwise healthy. He is in a large daycare environment and has three older siblings under the age of 6.
- Probable recurrent viral croup.
- Must consider the possibility of an underlying anatomic abnormality of the subglottis. AP and lateral neck/chest films are indicated. Strongly consider endoscopy to visualize and stage the subglottis if films are positive or croup continues.
- Inflammatory disorder: A 6-year-old with multiple known food allergies and a history of asthma and atopy presents to the emergency room in severe respiratory distress. He was well until lunchtime when he apparently sampled his friend’s ice cream bar that may have contained nuts. He presents with signs and symptoms of shock with pallor, cyanosis, palpitations, tachycardia, tachypnea, hypotension, wheezing, inspiratory stridor, and has pruritis and urticaria.
- Probable anaphylactic reaction (type 1) due to severe peanut allergy associated with allergic angioedema mediated by IgE antibodies.
- Treatment must include securing the airway, epinephrine, H2 blockers, antihistamines, fluid resuscitation, corticosteroids, and removal of the source of the anaphylaxis reaction, if applicable. Prevention of subsequent episodes is critical with identification of the allergen.
- RRP: A 2-year-old girl presents to the emergency room with progressively increasing stridor with activity and persistent dysphonia. She is the first-born child of a then 17-year-old mother, delivered vaginally without problems in the delivery suite. Mom has had an abnormal pap smear but denies condylomata. The child has been labeled as “asthmatic” and has made several previous visits to the emergency department and was treated with bronchodilators. At the present time she is in mild distress with use of accessory muscles of respiration but no air hunger, cyanosis, or dyspnea. Her pulse oximetry reads 100% saturation.

- Probable laryngeal papillomatosis.
- Treatment requires visualization of larynx and biopsy if appropriate. In a 2-year-old with mild distress this is best accomplished in a controlled setting (the operating room [OR]) with appropriate equipment and personnel readily available. The child needs to be consented for airway endoscopy and possible removal of papillomas and the mother needs to be counseled regarding the recurrent nature of these lesions. The OR needs to be properly set up in advance and the OR team and anesthesia team, along with the surgeon, need to discuss the sequence of events and the equipment that will be utilized before the child enters the OR.
- Laryngeal stenosis: A 27-week ex-preemie, born at 900 grams with severe BPD status/post a tracheotomy done at 10 weeks of age for failure to extubate, presents to you at 11 months of age for evaluation. The child is no longer requiring oxygen, has gained weight up to 8 kg, has GERD controlled on medications, and is no longer on bronchodilators. Endoscopy reveals an eccentric narrowing at the level of the cricoid and first tracheal ring along with a large suprastomal granuloma, with narrowing estimated at about 85% and predominantly anterior.

- Cotton class III subglottic stenosis, acquired.
- Treatment at this time would involve consideration of a single-stage laryngotracheal reconstruction with autologous costal cartilage grafting. Need to make certain that the GERD is under optimal control, that the child’s pulmonary reserve is adequate, and that all other medical conditions are stable before proceeding with reconstruction.
Complications
- Understand that acquired laryngotracheal disorders, such as subglottic stenosis, recurrent respiratory papillomatosis and infectious and inflammatory disorders of the larynx, carry with them the inherent complication of airway compromise.
- Know that it is imperative that the airway is secured and that the means to safely secure the airway are available as the first step in managing these disorders.
- Understand that a tracheotomy may be the most conservative operation to perform.
- Recognize the signs and symptoms of impending airway compromise.
- Formulate a plan to secure the airway before instrumenting it.
- Discuss the plan with other OR personnel.
- Know the importance of having proper equipment available and set up before beginning an airway procedure.
- Recognize the most common side effects of the medications used to treat infectious and inflammatory disorders of the larynx, including the signs, symptoms, and causes of anaphylaxis.
- Know to provide informed consent, including the potential need for placement of an alternative airway and postop monitoring in the intensive care unit to parents before engaging in airway surgery to prevent malpractice situations from occurring because of misunderstanding on the parents’ part regarding the severity of their child’s condition.
- Albert D, Leighton S. Stridor and airway management. In: Cummings CW, Haughey BH , Harker LA, et al., editors. Pediatric otolaryngology head & neck surgery. 4th ed. St. Louis: Mosby; 2004. p. 285-302.check pages
- Cotton RT. Management and prevention of subglottic stenosis in infants and children. In: Bluestone CD, Stool SE, editors. Pediatric otolaryngology. 4th ed. 2002, WB Saunders, Philadelphia. p. 1194-204. check pages
- Pransky SM. Evaluation of the compromised neonatal airway. Pediatr Clin North Am 1989;36:1571-83.
- Rutter MJ, Cotton RT. Laryngeal stenosis. In: Bailey BJ, editor. Head and neck surgery – otolaryngology. 4th ed.Philadelphia: Lippincott Williams & Wilkins; 2006. p. 881-93.chck pages
- Willging JP, Cotton RT. Subglottic stenosis in the pediatric patient. In: Myer CM, Cotton RT, Shott SR, editors. The pediatric airway: an interdisciplinary approach. Philadelphia: JB Lippincott; 1995. p. 111-32.
- Zalzal GH. Stridor and airway compromise. Pediatr Clin North Am 1989;36:1389-401.
Learner must Sign In to access AAO-HNSF education activities